Serum β-hCG Levels in Pregnant Women with Mild and Severe Preeclampsia During the Third Trimester
DOI:
https://doi.org/10.54133/ajms.v5i1S.398Keywords:
β-hCG, Complications, Maternal outcome, Preeclampsia, PregnancyAbstract
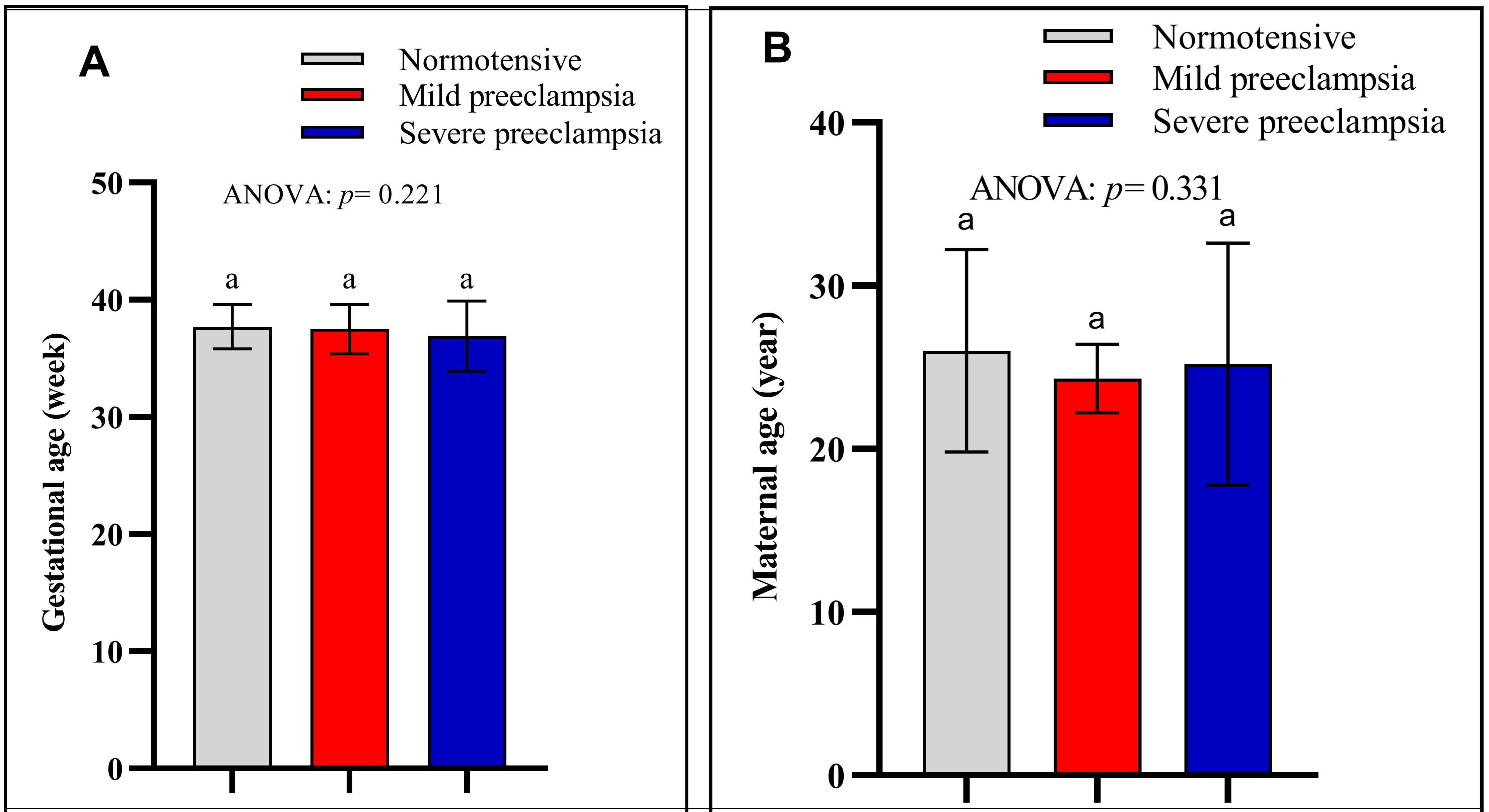
Background: Preeclampsia is a prevalent complication that frequently arises during pregnancy. It is a disorder of the trophoblasts. Given that human chorionic gonadotropin is secreted by the trophoblast, this complication may have an impact on its serum concentration. Objective: To compare the β-hCG levels of expectant women who are preeclamptic and those who are normotensive. Methods: A prospective cross-sectional study design was implemented at Al-Elweyia Maternity Teaching Hospital for this investigation. One hundred fifty expectant women in their third trimester are participating. The study participants were allocated into three cohorts, each consisting of 50 women: normotensive, mild preeclamptic, and severe preeclamptic. β-hCG levels in maternal serum were determined using an enzyme-linked immunosorbent assay (ELISA) in every instance. Results: Compared to expectant women with normotensive conditions and patients with mild preeclampsia, the levels of maternal serum β-hCG were significantly elevated in patients with severe preeclampsia. β-hCG levels were not significantly affected by maternal age across all three groups. Conclusion: β-hCG concentrations are greater in pregnant women with moderate and severe preeclampsia compared to normotensive women, with severe preeclampsia being more pronounced than mild.
Downloads
References
Lim R, Barker G, Lappas M. TREM-1 expression is increased in human placentas from severe early-onset preeclamptic pregnancies where it may be involved in syncytialization. Reprod Sci (Thousand Oaks Calif.). 2014;21:562–572. doi: 10.1177/1933719113503406.
Nikolic A, Cabarkapa V, Novakov Mikic A, Jakovljević A, Stosic Z. Ceruloplasmin and antioxidative enzymes in pre-Eclampsia. J Maternal-Fetal Neonatal Med. 2016;29:2987–2993. doi: 10.3109/14767058.2015.1111333.
Novakov Mikic A, Cabarkapa V, Nikolic A, Maric D, Brkic S, Mitic G, et al. Cystatin C in pre-eclampsia. J Maternal-Fetal Neonatal Med. 2012;25:961–965. doi: 10.3109/14767058.2011.601366.
Tranquilli AL, Dekker G, Magee L, Roberts J, Sibai BM, Steyn W, et al. The classification, diagnosis and management of the hypertensive disorders of pregnancy: A revised statement from the ISSHP. Pregnancy Hypertension. 2014;4:97–104. doi: 10.1016/j.preghy.2014.02.001.
Al-Jameil N, Tabassum H, Ali MN, Qadeer MA, Khan FA, Al-Rashed M. Correlation between serum trace elements and risk of preeclampsia: A case controlled study in Riyadh, Saudi Arabia. Saudi J Biol Sci. 2017;24:1142–118.doi: 10.1016/j.sjbs.2015.02.009.
Ugwuja EI, Famurewa AC, Ikaraoha CI. Comparison of serum calcium and magnesium between preeclamptic and normotensive pregnant nigerian women in Abakaliki, Nigeria. Ann Med Health Sci Res. 2016;6:33–37.doi: 10.4103/2141-9248.180269.
Rolfo A, Giuffrida D, Nuzzo AM, Pierobon D, Cardaropoli S, Piccoli E, et al. Pro-inflammatory profile of preeclamptic placental mesenchymal stromal cells: New insights into the etiopathogenesis of preeclampsia. PloS One. 2013;8:e59403.doi: 10.1371/journal.pone.0059403.
Wortelboer EJ, Koster MP, Kuc S, Eijkemans MJ, Bilardo CM, Schielen PC, et al. Longitudinal trends in fetoplacental biochemical markers, uterine artery pulsatility index and maternal blood pressure during the first trimester of pregnancy. Ultrasound Obstetrics Gynecol. 2011;38:383–388. doi: 10.1002/uog.9029.
Liu HQ, Wang YH, Wang LL, Hao M. Predictive value of free β-hCG multiple of the median for women with preeclampsia. Gynecologic Obstetric Invest. 2015;81:137–47.doi: 10.1159/000433434.
Ding X, Yang KL. Antibody-Free Detection of Human Chorionic Gonadotropin by Use of Liquid Crystals. Analytical Chem. 2013;85:10710–10716.doi: 10.1021/ac400732n.
El-Baradie SM, Mahmoud M, Makhlouf HH. Elevated serum levels of interleukin-15, interleukin-16, and human chorionic gonadotropin in women with preeclampsia. J Obstetrics Gynaecol Can. 2009;31:142–148.doi: 10.1016/s1701-2163(16)34098-1.
Karahasanovic A, Sørensen S, Nilas L. First trimester pregnancy-associated plasma protein A and human chorionic gonadotropin-beta in early and late pre-eclampsia. Clin Chem Lab Med. 2014;52:521–525.doi: 10.1515/cclm-2013-0338.
Zheng Q, Deng Y, Zhong S, Shi Y. Human chorionic gonadotropin, fetal sex and risk of Hhypertensive disorders of pregnancy: A nested case-control study. Pregnancy Hypertension. 2016;6:17–21. doi: 10.1016/j.preghy.2016.01.006.
Lee LC, Sheu BC, Shau WY, Liu DM, Lai TJ, Lee YH, et al. Mid-trimester beta-hCG levels incorporated in a multifactorial model for the prediction of severe pre-eclampsia. Prenatal Diagnosis. 2000;20:738–743. doi: 10.1002/1097-0223(200009)20:9<738::aid-pd917>3.0.co;2-r.
Long W, Zhou Q, Wang H, Lu B, Chen Y, Zhang B, et al. Second-trimester maternal serum screening biomarkers in the risk assessment for preeclampsia. Ann Clin Lab Sci. 2018;48:308–313. PMID: 29970433.
Papastefanou I, Chrelias C, Siristatidis C, Kappou D, Eleftheriades M, Kassanos D. Placental volume at 11 to 14 gestational weeks in pregnancies complicated with fetal growth restriction and preeclampsia. Prenatal Diagnosis. 2018;38:928–935.doi: 10.1002/pd.5356.
Yu N, Cui H, Chen X, Chang Y. First trimester maternal serum analytes and second trimester uterine artery doppler in the prediction of preeclampsia and fetal growth restriction. Taiwanese J Obstetrics Gynecol. 2017;56:358–361.doi: 10.1016/j.tjog.2017.01.009.
Kim SY, Kim HJ, Park SY, Han YJ, Choi JS, Ryu HM. Early prediction of hypertensive disorders of pregnancy using cell-free fetal DNA, cell-free total DNA, and biochemical markers. Fetal Diagnosis Ther. 2016;40:255–262.doi: 10.1159/000444524.
Opichka MA, Rappelt MW, Gutterman DD, Grobe JL, McIntosh JJ. Vascular dysfunction in preeclampsia. Cells. 2021;10(11):3055. doi: 10.3390/cells10113055.
Fisher SJ. Why is placentation abnormal in preeclampsia? Am J Obstet Gynecol. 2015;213(4 Suppl):S115-22. doi: 10.1016/j.ajog.2015.08.042.
Zahra Basirat Z, Barat S. Serum beta-human chorionic gonadotropin levels and preeclampsia. Saudi Med J. 2006;27(7):1001-1004.
Dugoff L, Hobbins JC, Malone FD, Porter TF, Luthy D, Comstock CH, et al. First-trimester maternal serum PAPP-A and free-beta subunit human chorionic gonadotropin concentrations and nuchal translucency are associated with obstetric complications: a population-based screening study (the FASTER Trial). Am J Obstet Gynecol. 2004;191(4):1446-1451. doi: 10.1016/j.ajog.2004.06.052.
Khanam Z, Mittal P, Suri J. Does the addition of serum PAPP-A and β-hCG improve the predictive value of uterine artery pulsatility index for preeclampsia at 11–14 weeks of gestation? A prospective observational study. J Obstet Gynecol India 2021;71:226–234. doi: 10.1007/s13224-020-01420-7.
Erez O, Romero R, Maymon E, Chaemsaithong P, Done B, Pacora P, et al. The prediction of late-onset preeclampsia: Results from a longitudinal proteomics study. PLoS One. 2017;12(7):e0181468. doi: 10.1371/journal.pone.0181468.
Yadav K, Aggarwal S, Verma K. Serum βhCG and lipid profile in early second trimester as predictors of pregnancy-induced hypertension. J Obstet Gynaecol India. 2014;64(3):169-174. doi: 10.1007/s13224-013-0490-3.
Gurbuz A, Karateke A, Mengulluoglu M, Gedikbasi A, Ozturkmen M, Kabaca C, et al. Can serum HCG values be used in the differential diagnosis of pregnancy complicated by hypertension? Hypertens Pregnancy. 2004;23(1):1-12. doi: 10.1081/PRG-120028276.
Danielli M, Thomas RC, Gillies CL, Hu J, Khunti K, Tan BK. Blood biomarkers to predict the onset of pre-eclampsia: A systematic review and meta-analysis. Heliyon. 2022;8(11):e11226. doi: 10.1016/j.heliyon.2022.e11226.
Chang KJ, Seow KM, Chen KH. Preeclampsia: Recent advances in predicting, preventing, and managing the maternal and fetal life-threatening condition. Int J Environ Res Public Health. 2023;20(4):2994. doi: 10.3390/ijerph20042994.
Rybak-Krzyszkowska M, Staniczek J, Kondracka A, Bogusławska J, Kwiatkowski S, Góra T, et al. From biomarkers to the molecular mechanism of preeclampsia-A comprehensive literature review. Int J Mol Sci. 2023;24(17):13252. doi: 10.3390/ijms241713252.
Kasraeian M, Asadi N, Vafaei H, Zamanpour T, Shahraki HR, Bazrafshan K. Evaluation of serum biomarkers for detection of preeclampsia severity in pregnant women. Pak J Med Sci. 2018;34(4):869-873. doi: 10.12669/pjms.344.14393.
Han L, Holland OJ, Da Silva Costa F, Perkins AV. Potential biomarkers for late-onset and term preeclampsia: A scoping review. Front Physiol. 2023;14:1143543. doi: 10.3389/fphys.2023.1143543.
Eskild A, Strøm-Roum EM, Haavaldsen C. Does the biological response to fetal hypoxia involve angiogenesis, placental enlargement and preeclampsia? Paediatr Perinat Epidemiol. 2016;30(3):305-309. doi: 10.1111/ppe.12283.
Downloads
Published
How to Cite
Issue
Section
License
Copyright (c) 2023 Al-Rafidain Journal of Medical Sciences ( ISSN 2789-3219 )

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Published by Al-Rafidain University College. This is an open access journal issued under the CC BY-NC-SA 4.0 license (https://creativecommons.org/licenses/by-nc-sa/4.0/).